My friend Matthias Schneider from Düsseldorf and I had occasion to exchange e-mails recently, as I’m looking to contact one of his former young charges who once was doing some interesting things with arthroscopy. When Matthias and a colleague visited Ann Arbor in the 90s, Kathy and I fed them dinner which featured the Caesar salad we’d learned to make from Kate, the waitress at the now defunct Lord Fox who used to make it for us at table side whenever we went there, which was often. Thanks to Mattthias’ urging (I’d been promising him the recipe for decades) the recipe is now on a Word file, not just the flimsy piece of pink paper Kate wrote it it on, which is in danger of disintegrating or being rendered unintelligible by one more spill. So now I get to share it with you. You’ll like it. It’s worth the fuss. Careful with the vinegar.
(thanks to Kate at the late lamented Lord Fox)
Caesar Salad
Start with a nice big wooden salad bowl
1 clove garlic
2 filets anchovies
1 tsp. Dijon mustard
dash or 2 Worcestershire sauce
2 drops Tabasco
½ to full way round bowl of wine vinegar (1/2 Tbsp)
What started as a meandering around various spots I’ve landed in medicine led to the realization I have a pretty famous (in some circles) Grandfather.
I was actually looking for symbols and crests. Some places I’ve been, like my medical school, have some pretty awesome crests. The back of my new business card has crests or seals from high school, U of C and Barnes Hospital. U of M doesn’t allow private use of its seal.
I had the privilege of studying in London part of my senior year in medical school. Should be some great seals and crests at those places, right?
My first rotation was in cardiology at St. George’s Hospital at Hyde Park Corner, S.W.1, the most expensive piece of real estate in London. The great white building dates to the early 1800s and was designed by the same architect that did the National Gallery
In the late 1800s, patients were rationed 3 pints of beer a day. The practice had fallen off by the time I got there. Indeed, I was there for its last days as a hospital. St. George’s medical school had been building in Tooting, SW17, a far less fashionable (and expensive) working class neighborhood 2 postal districts over from Wimbledon (SW19). Old St. George’s became a luxury hotel in 1980. I stayed in Tooting and took the train into Hyde Park. The man I came to follow – Dr. Aubrey Leatham – was one of the greats of his generation https://www.thetimes.co.uk/article/dr-aubrey-leatham-lwrqqhs0vt7
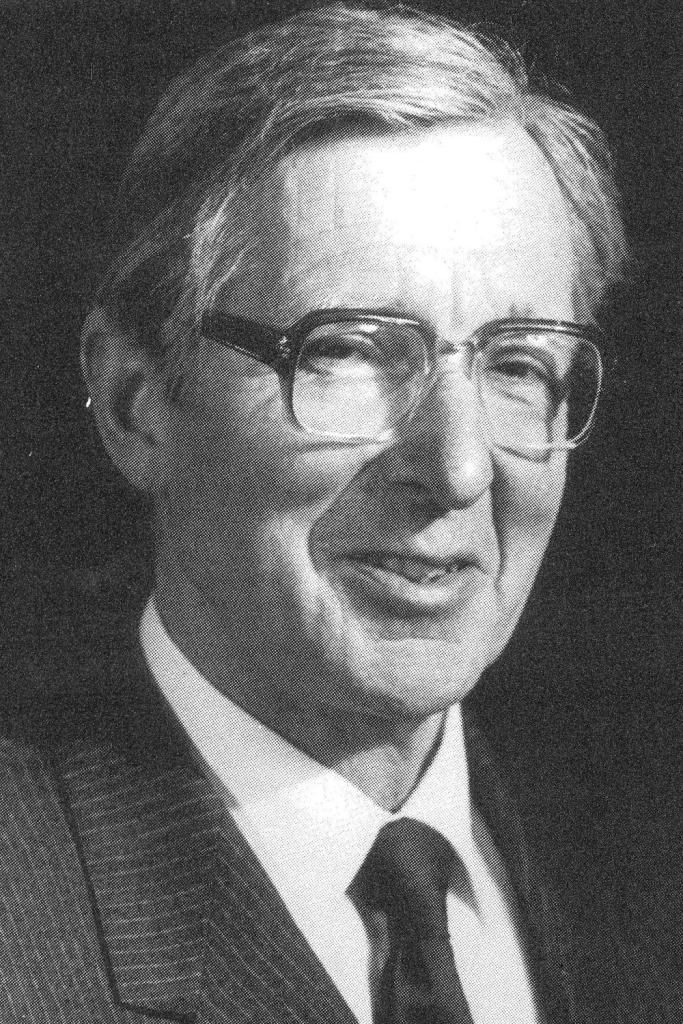
He brought bedside auscultation (listing to the heart) from an art to a science by comparing what the doctor said he heard to what a machine recorded (phonocardiography). The main attractions to me in cardiology (and they were strong attractions) were the bedside exam and electrocardiography. I came to London as that is where the bedside exam is still well taught and revered. Dr. Leatham was gentlemanly, precise, encouraging, and charismatic. I felt privileged to be included in the small crowd following him around. He’d invented a somewhat complicated and awkward stethoscope https://www.worthpoint.com/worthopedia/leatham-stethoscope-1813889663 which I did not buy as I liked my simple Littman. Now WorthPoint states it’s “arguably the finest stethoscope ever made”. Would have made a great conversation piece. And Professor Leatham was a distinguished looking fellow
My request for a place on his team was guided by my Professor at U of C, Leon Resnekov, then the star of the Cardiology Division, but very much involved in the teaching of this particular student: attentative, critical, demanding but encouraging. He even made special arrangements to see my nurse girlfriend after I heard a click-murmur (she indeed did have mitral valve prolapse). He knew of my independent wanderings with my friend and classmate Marty Sanders chasing down patients rumored to have interesting auscultatory findings. He died young 14 years after I graduated, at 65. http://chronicle.uchicago.edu/930930/resnekov.shtml
Both Drs. Resenekov and Leatham passed through the National Heart Hospital in their training. Dr. Resnekov came from Cape Town, one of several talented South Africans on faculty at U of C. My class even did a bit on them in our Senior Skit. Dr. Leatham spent his life on the Island.
The man who trained them both had been born of a British father in India, grew up in New Zealand, going to medical school – struggling sometimes – in Melbourne, before going back to Christchurch to start. He clamored his way into the London hospitals and dazzled all he encountered, except for those who disliked his criticism of the older methods he found lazier and sloppier. He became the most renowned British cardiologist of the 20th century: Paul Wood.
Dr. Wood died of an MI in 1962 at age 55. He’d asked not to be resuscitated, which in those days would have involved cutting open his chest to massage his heart. Defibrillators were a few years off. Detractors blamed his insistence on being anticoagulated with heparin – controversial them – possibly taking a pericarditis situation into tamponade. His autopsy showed a solitary obstruction in his left anterior descending artery: a widowmaker.
It was only while putting this information together to tell Mike Shea, Michigan Medicine’s finest cardiologist and a good friend and colleague of many years, that I realized the connections. Mike spent a couple of years in London early in his career and appreciates the British tradition in Cardiology.
Mike had met Dr. Leatham. He did not know Dr. Resnekov. When I realized my cardiology mentors were from the Paul Wood line, I asked Mike if I could claim lineage. Mike assured me I could. From a straight shooter like Mike, with his great respect for the British way and Paul Wood (he still has a copy of Paul Wood’s textbook, published in the 50s), I’ll take that as an endorsement. So, it’s like finding out you have a grandfather you never knew you had. And a famous one at that. Thank you, Dr. Wood. Had cardiology remained just what you taught, with careful bedside assessment and scrutiny of the heart’s electrical signals, I might have joined your many grandsons in the field. But the catheters you were beginning to employ to fine tune physiologic assessments became brute force tools for assessment and correction of plumbing while high stakes life-and-death scenarios became the norm. Rheumatology has been a much better fit, but careful listening serves this field well also, and I learned that on cardiology.
On March 30th, in plenty of time to avoid being taken for an April Fool’s joke, California Governor Gavin Newsome issued executive order N-39-20 https://www.gov.ca.gov/wp-content/uploads/2020/03/3.30.20-EO-N-39-20-text.pdf giving the Director of the Department of Consumer Affairs (DCA) the authority to waive professional licensing requirements for the healing arts boards under DCA during the COVID-19 State of Emergency. Any medical professional (doctors, dentists, nurses, respiratory therapists, physical therapists, behavioral health scientists, pharmacists, EMTs) who have had an active California license within the previous 5 years but have let it lapse can renew their license without charge. The license will be good for only 6 months (usual term of renewal is 2 years) and is contingent on registration with the new California Health Corps https://covid19.ca.gov/healthcorps/. Promise to new Corps members is a salary (although the amount is never mentioned) and malpractice insurance. Applicants can state regional preferences for posting, and will have their skill sets screened so as to match needs as best possible. The main mission of this new army will be to staff an additional 50,000 hospital beds, now closed, but expected to be needed as the COVID-19 pandemic spreads. The state has reported over 6,000 cases already, figuring that to be a gross underestimation due to spotty testing. As of last Monday, 1432 cases were in hospital, over 600 of those in intensive care https://www.nytimes.com/2020/03/31/us/california-health-corps-newsom.html. Today’s Johns Hopkins map https://coronavirus.jhu.edu/map.html shows 5,304 confirmed cases in Los Angeles alone.
The pool is deep. Over 37,000 medical professionals had a California license sometime in the past 5 years but let it lapse. I’m one of them. I got a California Medical License in late 2016 in anticipation of my sabbatical at University of California at San Diego, which ran from January through the end of March. When the time to renew came last year, I balked at paying the high fee ($820, more than twice what it costs in Michigan, which is good for twice as long). When the post at UCSD did not materialize, and my medical career seemed destined to remain firmly planted in Michigan, one license seemed sufficient. Even if I could secure a Corps posting in La Jolla, I think I’ll hold off on my return to the Golden State till the environment becomes less hazardous. If I eventually feel moved to stand on the front lines in this battle, there will be opportunities within walking distance
An article in the New York Times yesterday gave a face to a controversial treatment for COVID-19 that’s been the stuff of rumors for weeks https://www.nytimes.com/2020/04/02/technology/doctor-zelenko-coronavirus-drugs.html. Dr. Zev Zelenko, primary care doctor to his community of 35,000 Hadassic Jews in Kiryas Joel, about an hour’s drive from Manhattan, has been treating even mild cases with not only Plaquenil, but adding in zinc supplements and azithromycin (the stuff in your Z-Pac). Now doctors have been giving Z-Pacs to their patients with viral infections for years. Thought leaders in infectious disease warn against the practice, as the drug has no anti-viral activity and indiscriminate antibiotic use can spread drug resistance. Zinc is harmless, competes with viruses in some of the host proteins they try to hijack, and zinc lozenges are a staple in my medicine cabinet to pop in at the first sign of a scratchy throat.
Azithromycin is a popular, well known and well-studied antibiotic. It was derived from erythromycin, another antibiotic in the macrolide class. It prevents bacteria from growing by interfering with their protein synthesis. It binds to the 50S subunit of the bacterial ribosome and thus does not let bacterial messenger RNA latch on to the ribosmome and tell various amino acids to start hooking together into a new protein. Macrolides have also been shown to have immune-modulating and anti-inflammatory effects. Morbidity and mortality caused by respiratory viral infections is associated more with an overexuberant host response, with the excessive elaboration of cytokines and immunopathologic host inflammatory responses, than with direct effects of the virus. Pre-clinical and clinical studies have shown that macrolides diminish the inflammatory response, attenuating extreme cytokine production and promote the induction of immune protein antibodies which may reduce the complications of respiratory viral infections. Given these properties, macrolides (e.g., azithromycin, clarithromycin, erythromycin, fidaxomicin, telithromycin) have been studied for their potential use as targeted therapy for a wide spectrum of viral respiratory infections including influenza. Results from studies in these various diseases have been mixed. There seems to be a positive influence on the course of kids with flu or respiratory syncytial virus (RSV, a common cause of pneumonia in kids), but not on adults with flu.
In the 2012 MERS epidemic in Saudi Arabia, caused by a coronavirus 87% identical to COVID-19, doctors used a lot of azithromycin, but in no consistent manner. In a paper published just last year, 26 authors in service to the Saudi Clinical Trials Group looked back on outcomes of 349 critically ill MERS patients, which included 136 who had received macrolides (azithromycin the most common, used in 72%). The group could find no evidence that antibiotics reduced 90 day mortality or shortened the duration that virus was shed by the patients.
While these results seem to put a damper on any enthusiasm for azithromycin in COVID-19, realize the Saudi patients were critically ill, and that might get a COVID-19 patient high dose steroids or even an interleukin-6 inhibitor, like Actemra. Dr. Zelenko’s patients weren’t nearly as sick, and no doubt were grateful for any shortening of symptoms they thought his treatment was providing. Did he keep some out of the ICU? With the large population of new infected patients, a proper trial comparing Plaquenil alone to Plaquenil plus a Z-Pac, with monitoring of viral shedding as well as symptoms, seems eminently doable, especially with our huge medical research infrastructure. Let’s get to it, Dr. Fauci!
Arabi YM, Deeb AM, Al-Hameed F, Mandourah Y, Almekhlafi GA, Sindi AA, Al-Omari A, Shalhoub S, Mady A, Alraddadi B, Almotairi A, Al Khatib K, Abdulmomen A, Qushmaq I, Solaiman O, Al-Aithan AM, Al-Raddadi R, Ragab A, Al Harthy A, Kharaba A, Jose J, Dabbagh T, Fowler RA, Balkhy HH, Merson L, Hayden FG; Saudi Critical Care Trials group. Macrolides in critically ill patients with Middle East Respiratory Syndrome. Int J Infect Dis. 2019 Apr;81:184-190. doi: 10.1016/j.ijid.2019.01.041. Epub 2019 Jan 25.
On Sunday, the Food and Drug Administration (FDA) issued an Emergency Use Authorization (EUA) to the Health and Human Services’(HHS) Office of the Assistant Secretary for Preparedness and Response Biomedical Advanced Research and Development Authority (ASPAR’s BARDA) for hydroxychloroquine and chloroquine for coronavirus treatment. The agency allowed for the drugs to be “donated to the Strategic National Stockpile to be distributed and prescribed by doctors to hospitalized teen and adult patients with COVID-19, as appropriate, when a clinical trial is not available or feasible,” HHS announced https://www.hhs.gov/about/news/2020/03/29/hhs-accepts-donations-of-medicine-to-strategic-national-stockpile-as-possible-treatments-for-covid-19-patients.html that Sandoz had donated 30 million doses of hydroxychloroquine to the stockpile and Bayer donated 1 million doses of chloroquine.
From HHS’ announcement: “An EUA may be issued if the FDA determines that, among other criteria, the known and potential benefits of the product, when used to diagnose, prevent, or treat the identified disease or condition, outweigh the known and potential risks of the product, and there are no adequate, approved, available alternatives. Emergency access to a medical product under an EUA is separate from use of a medical product under an investigational drug application.” Other than a requirement that doctors prescribing the drug be given a sheet explaining risks and drug interactions, there are no further restrictions on doctors. The donation of supplies by pharma merely eases the supply crunch but does not make the drugs free.
As of this Monday morning, the FDA had not yet mentioned this move on its site.
Thus, any doctor treating a patient with COVID-19 will be able to prescribe one of these drugs without fear of legal repercussions for use of an “unapproved drug”. News of the announcement came on Politico https://www.politico.com/news/2020/03/29/fda-emergency-authorization-anti-malaria-drug-155095, which of course tries to put a political spin on the move, which was championed by the White House and has no lack of detractors.
This is very good news, and only took 5 acronyms to explain. Good thing NASA isn’t handling the problem.
I thought after all this coronavirus stuff, we needed a light break. As is often the case these days, this one was inspired by my high school English teacher Mrs. Pharriss. Towards the end of a long e-mail, she asked me:
“Did you have to deal with deaths of patients very often during your medical career? How did you deal with it? I should read more about your field—I think I have an old Merck Manual on a bookshelf somewhere—to understand the kinds of diseases you must have treated. You’ve mentioned lupus, one other rather rare one that your high school friend had, of course, arthritis. Why did you choose this area of medicine? “
To which I responded:
Dear teacher
Is this an essay assignment or a test you’ve given me? These questions you’ve asked are very heavy and deep ones. Let’s start with choice of rheumatology. The subspecialty is a constant game of Trivial Pursuit and Clue. I was introduced in second year of medical school when the local rheumatology faculty delivered us 2 series of lectures. I was immediately fascinated by the weird array of strange and often rare diseases they looked after. I had never heard anything like it. I spent some time with the chief of rheumatology, Leif Sorensen (what a name!) in my senior year, not only seeing some of these oddball diseases up close, but learning it was sometimes possible to do something about them. It didn’t hurt that my dear grandma Slater had bad arthritis, boring old osteoarthritis of the knees (OAK), but maybe I yearned to be able to do something about that. Curiously, much of my research effort early on at Michigan focused on OAK and my major procedural efforts, for which I became renowned, over the course of my career focused mainly on OAK. Barnes provided plenty of distractions to do something else with my talents. Pulmonary medicine was attractive, as the docs in that field were quite affable and we had fun at conferences. Gastroenterology had its pull, as it does for many medical residents to this day, not for the prospect of doing high-paying procedures, but for the interesting disorders involving the liver and inflammation of the gastrointestinal tract. I’d enjoyed cardiology in med school, mainly the games of trying to sort out a patient’s heart problem by listening to the sounds it makes and discerning perturbations in the heart’s electrical system by scrutinizing the squiggles on EKG paper; but the life and death heroics of the CCU were not for me. When I took rotations with the legendary Bevra Hahn, who did not like me as I occasionally left her late afternoon rounds to go to my moonlighting job, I got hooked back into rheumatology. The fellowship programs I chose to seek were narrow and pretty high powered: UCSF, Hopkins, Barnes and Michigan. I got little love after visiting UCSF and Hopkins, and Barnes’ young new chief John P. Atkinson (with whom I am still friends) said he would not be able to offer me a slot. I had been quite the bad boy at Barnes and the reputation stuck. Only dear old Giles G. Bole took a chance on me at U of M and the relationship became a solid and fulfilling one. They thought I was terrific (I was) and offered me a job midway through my second fellowship year. As the young stud steeped in the fires of Barnes, I took on everything. Rheumatologists are called in not only when a patient with one of their established diseases lands in the hospital, but also when a particular patient has a complex array of symptoms and signs that just might have an autoimmune basis. I quickly developed a reputation as the guy who didn’t believe any of the other consultants. But our patients were different! It led to some clashes with the powers that be which were to punctuate the rest of my career. I learned to lighten up and realize that the effective consultant could persuade others to see his, correct, point of view. The practice of rheumatology became much easier in the late 90s with the advent of biologicals. These drugs actually worked great, and I wouldn’t have to spend each visit deciding which inflamed joints to inject. Some of the joy of rheumatology began to fade in the last decade or so, as the practice became increasingly corporatized. Large committees began to decide what constitutes a particular disease, and how best to treat it. Protocols deigned what to do with our patients, and the satisfaction of figuring things out independently and devising something clever to do about it faded. With protocols came overseers to see that you adhered to them, and who likes someone looking over your shoulder? So while I was sad to be forced to give up my practice in 2019, I really wasn’t having that much fun anymore and I’m not terribly sad it’s all gone.
Deaths are rare in Rheumatology. Our patients die with their diseases, not of them. We docs are blamed for killing them early, with NSAIDs, opioids, and the myriad biologics permitting all manner of weird infections. On the consult service, we see our share of deaths, mainly inpatients with multisystem diseases who just become overwhelmed. I came to tears thinking about your questions while preparing dinner. It helped I was chopping up a big sweet onion at the time (the sauce turned out delicious). I thought back to patient deaths that hit me. There have been a bunch, but that of Sylvia Fryer particularly haunts. She was a middle-aged woman from a small town outside of Jackson who had hepatitis C, before anyone knew what that was, except me. She had a rare complication of hepatitis C infection called cryoglobulinemia, in which an excessive immune response to the virus includes some immune proteins that tend to glom up at lower temperatures. The proteins deposit in critical organs and cause all sorts of trouble. I was able to bring Sylvia along for a while, but things inevitably progressed. I recall sitting at her bedside in the ICU, she on a ventilator, me holding her hand thinking how unfair it was she was dying, as she’d fought so hard. Current hepatitis C drugs would probably have cured her. Maybe that’s my best death story. I think I’ve killed only one patient with opioids, one middle aged guy with hepatitis C and joint pain whom I’d strung along with huge amounts of opioids who just stopped showing up one day. A couple years ago I learned of the sudden death of an older patient with bad rheumatoid arthritis for whom I’d been prescribing a modest chronic dose of opioids. She had other reasons to keel over. Those deaths may be more troubling than the ones in hospital, where someone somewhere might think you had a hand. I realize I entered this profession with a license to kill, but I didn’t intend to apply it. As Hippocrates wrote Primum non nocere
The Department of Internal Medicine (my home) at the University of Michigan Medical Center devoted its weekly Grand Rounds to a discussion of the first 30 days of COVID-19 here.
Just last week, the hospital opened a new ward – the 32 bed RICU (Regional Infectious Containment Unit) – devoted to the care of COVID-19 patients, featuring negative pressure to keep materials from spreading beyond the unit. The unit quickly filled and now encompasses 50 beds, devoted now only to the most serious cases. The second patient ever encountered was a middle aged woman with lupus, Sjögren’s and preexisting lung disease who was already on Plaquenil plus some more potent immunosuppression. In anticipation of compassionate use of the experimental antiviral remdesivir, she had her Plaquenil held, and she became rapidly worse, only to have the Plaquenil reinstated. Despite continued Plaquenil, remdesivir, Actemra and steroids she remains on the ventilator at maximum support, still alive.
One huge leap forward was getting our own high throughput lab testing for coronavirus, not having to rely on sendouts or the low capacity CDC test.
Treatments pretty much follow the guidelines I’ve shared with you out of China on my blogs. They do start Plaquenil a little higher, 600 mg twice daily vs. 400 mg, but otherwise dose it the same. One new drug to creep onto the list of options is nitazoxanide (Alinia), approved by the FDA in 2004 for treatment of protozoal infections (cryptosporidiosis and giardia, both water borne buggers that can cause diarrhea, with crypto having become a particular problem in HIV patients). It works by interfering with the pyruvate ferredoxin/flavodoxin oxidoreductase dependent electron transfer reaction, which is essential to anaerobic energy metabolism. As such, it markedly modulates the survival, growth, and proliferation of a range of extracellular and intracellular protozoa, helminths, anaerobic and microaerophilic bacteria, in addition to viruses. Nitazoxanide exhibited activity against the MERS coronavirus in the test tube, but there have been no reports of its clinical efficacy.
Three clinical trials are in progress at U of M. Two employ remdesivir, one for moderate illness and one for severe illness. Another employs sarlilumab (Kevzara), an anti-interleukin-6 monoclonal antibody, very similar to tocilizumab (Actemra), which I’ve discussed before.
So we plug along at U of M, looking to face a flood of new cases over the next 2 weeks. They haven’t yet begun trying to coax the retirees back into harness, at least yet. Stay tuned.
actually, those 95 authors did provide a table of the drugs they’ve tested which show promise against coronavirus. Here it is. I fear the structure of the table has not survived the paste. I refer the interested reader back to the URL in my last blog post. Take it as a demonstration of the amazing array of stuff out that that may be able to corral our annoying little visitor.
Table 1a. Literature-deriveda drugs and reagents that modulate SARS-Cov-2 interactors.
Ca2+ channel inhibitor and drug efflux transporter inhibitor
Ki = 113
AZ3451137 F2RL1 Orf9c Pre-clinical
PAR2 negative allosteric modulator pKD = 15
These drug-target associations are drawn from chemoinformatic searches of the literature, drawing on databases such as ChEMBL141, ZINC142 and IUPHAR/BPS Guide to Pharmacology143
Table 1b. Expert-identifieda drugs and reagents that modulate SARS-CoV-2 interactors.
Compound Name
Compound Structure
Human Gene/ Process
Viral Bait
Drug Status
Activity (nM)
ABBV-74468 BRD2/4 E Clinical Trial
Degrades BRD BRD2/4 E Pre-clinical proteins IC50 < 10000
a. These molecules derive from expert analysis of human protein interactors of SARS-Co-V2 and reagents and drugs that modulate them; not readily available from the chemoinformatically-searchable literature.
The latest piece of COVID-19 information circulating in my Division Monday was a pre-print of a manuscript submitted to Nature (perhaps the world’s most highly regarded scientific journal) regarding the results of a molecular tour de force investigation of COVID-19’s protein components and the human proteins with which they interact, examining properties of existing drugs which might disturb those interactions and thereby cripple the virus. The paper has not finished going through the peer-review process, so the final “official” report could end up looking slightly different.
There are 95 authors listed in the masthead, almost all with various UCSF associations, but Paris, Seattle and New York City are also represented.
They started by taking the virus apart. That 30,000 base pair RNA genome has 14 ”open reading frames” you could call genes which direct synthesis of 14 globs of protein which manage to self digest and reassemble themselves into 16 non-structural proteins (which direct the virus’ dirty work on the cell), 4 structural proteins (which the virus presents to the world in its “crown”) and 9 “accessory factors” which have a mysterious role. They managed to clone all 29 of these into plasmids (DNA taken up by cells and expressed) and gotten cultured human cells to crank out good amounts of each one. They could verify each product was the real deal in 27 instances. Then they mixed them up with proteins from human cells from 16 different organs coronavirus is known to infect. The identified 332 interactions between different virus proteins and different cell materials. Here is where the rubber was meeting the road when coronavirus sets up shop. Interfere with those interactions and maybe you’ve got a chance. To be more sure that the human proteins interacting in the test tube were relevant, they checked the evolutionary profiles of the proteins, judging that proteins more stable across evolution would more likely be real viral targets. The 332 looked like they filled this bill. They characterized the nature of the various interactions, finding interactions related to lipid modifications and vesicle trafficking (the virus moves in and out of intracellular vesicles and appropriates the cell’s lipids for its own coat), interactions with multiple innate immune pathways (the defenses our cells have at the ready regardless of identity of invader), interactions with a Cullin ubiquitin ligase complex (don’t ask me), and interaction with bromodomain proteins (important in regulating gene transcription).
Then came the “wow” part (if the molecular virology thusfar didn’t tickle you as much as it did this old virologist). They sought to find molecules that would target human proteins in the SARS-CoV-2 “interactome” (a term I think they just coined, but a nice way to describe whatever two-backed beast that formed whenever bits of corona and human came together). Drugs are no longer some sort of mystery potion drawn from the doctor’s bag. Molecular structures are known, and at least putative mechanisms exist. And they’re all catalogued. Chemoinformatics, they call it. They found 62 drugs that could conceivably modulate the virus-human interactions they’d characterized. Some are still pre-clinical. But some old war horses showed up, including Depekote (valproic acid), an anti-seizure drug, Haldol (haloperidol), an anti-psychotic (which we might all need if this goes on much longer), chloroquine (Aralen) of course, CellCept (mycophenolic acid, an immune suppressant and anti-transplant drug), ribavirin (already in the Chinese guideline), and even metformin (a common diabetes drug). As I type this, I plan to make you a full table, which the 95 authors did not. I’m going to save that for a later post so I can get this out. There’s not a lot of room in Nature. Not a problem here, but I have your attention span to consider.
Please don’t go asking your doctor for any of these drugs. That’s happening badly enough with Plaquenil already. But realize this sort of high-tech investigation is going on and could rapidly lead to new treatments for our current plague. Trust that the nerds have their noses to the grindstone and good stuff is bound to turn up.
My young friend Jason, research superstar and damn fine doctor to boot (see “shameless plugs” 2/22/20), is married to Sara, a science writer. Sara has spent the last little while researching how the patients Jason and I look after see the new interest in one of their mainstay drugs – Plaquenil (hydroxychloroquine) – as a possible treatment for COVID-19. Several of my recent posts have devoted space to that, but Sara examines the point of view of those who feel threatened by this interest. I take the point of view that ramped up production should meet the needs of both rheumatology and coronavirus patients. Until now, the market for hydroxychloroquine was pretty stagnant and manufacturers had no reason to produce more.
Her article appears in Undark, an interesting non-profit, editorially independent digital magazine exploring the intersection of science and society, based in Cambridge Mass, where there’s a lot of that about (M.I.T., Harvard and all that). Here it is: https://undark.org/2020/03/22/hydroxychloroquine-lupus-covid19-coronavirus/