The Chinese Health and Public Health Ministry Guideline on Novel Coronavirus Disease (COVID-19) Diagnosis and Treatment (revision #6) was released in Beijing March 4th. The guideline derives from experiences in treating over 80,000 Chinese patients. The document has been translated from Mandarin and stealthily but broadly circulated for about a week. Dr. Ainlin Xu, an allergist in private practice in Silicon Valley who grew up in Shanghai, sent it to one of my colleagues – who emailed it to the rest of the Division on Saturday – and asked that anyone receiving it make the document available to “as many health institutions/hospitals/doctors as you can reach”. If you Google it, you won’t go anywhere near the actual document. But I’m pasting the whole thing in right here. Much of it is stuff we already know, but there are some pretty interesting bits, particularly as regards treatment. I’ll be commenting on that in my next post. So here ya go, all 9 pages of it:
The 3/4/2020 Chinese Health and Public Health Ministry Guideline on Novel Coronavirus Disease (COVID-19) Diagnosis and Treatment (Revision #6)
(I only summarized the clinically relevant information for US Healthcare System/Hospitals/Clinics)
- Characteristics of Pathogen
The Novel Coronavirus (2019-nCoV) belongs to the family of beta Coronavirus family. It has significant genetic differences from SARSr-CoV, and MERSr-CoV. Current research indicates that it has 85% genetic similarity with bat-SL-CoVZ45, isolated from bats. When cultured outside the human body, 2019-nCoV can be detected in human respiratory epithelial cell within 96 hours, and after 6 days in Vero E6 and Huh-7 cells.
The virus is sensitive to UV light and heat. Heat for 56C for 30min, Diethyl Ether, 75% Ethanol, disinfectant with chloride, H2O2, and other chlorinated disinfectant can effectively deactivate virus.
- Characteristic of Infectibility
- Origin of Infection
Currently the main source of Infections are patients infected with the virus. Patients without any clinical symptoms can also infect others.
Droplet and close contact are the main route of transmission. Within enclosed environment, long time exposure in high viral load situation, transmission through aerosol is possible. The Novel Coronavirus can be isolated in feces and urine. It can be transmitted through contact or aerosolized droplets through the infected patient’s feces or urine.
The general population (a supplemental guideline from the front line hospitals says most patients infected are adults 30 years or older)
- Clinical Presentation
Incubation Period is 1-14 days, most 3-7 days.
Fever, dry cough, fatigue are the primary symptoms. Some patients have nasal congestion, rhinorrhea, sore throat, muscle pain and diarrhea. Severe patients usually develop difficulty breathing and hypoxia 1 week after onset of symptoms. Critical patients may develop rapid progression into ARDS, sepsis, uncorrectable metabolic abnormality, DIC, and multi-organ failure. Notably, severe and critical patients can have low grade fever, or no fever at all.
Some children and newborns present with atypical symptoms, such as vomiting, diarrhea, or just malaise or shortness of breath. Children generally have milder symptoms.
Mild patients present with low grade fever, mild fatigue, etc., without any signs of pneumonia.
From current cases, majority of patients can recover well. Minority of patients become critical. Elderly patients and patients with baseline diseases have poorer recovery. Pregnant patients with COVID-19 have similar clinical courses as their non-pregnant peers.
(a supplemental guideline from the frontline hospitals says that it appears male have more severe diseases than female, and have a higher mortality rate)
In early stages of the disease, peripheral WBC number decreases, so is absolute lymphocytes. (A supplemental guideline from the frontline hospitals also says that absolute lymphocyte/absolute neutrophil ratio seems to have some value in determining the severity of a patient’s disease, and help to indicate trend in a patient’s condition. The lower the ratio, the more severe the patient is.)
Some patients have elevated liver enzymes, LDH, and Myoglobulin; some have elevated Troponin. Most patients have elevated CRP and ESR. Severe patients have elevated D-Dimer, suppressed peripheral lymphocytes. Severe and critical patients showed signs of elevated inflammatory mediators (cytokines, such as IL-6).
Virus can be detected through RC-PCR in patient’s nasopharyngeal swab, sputum, other lower airway secretions, blood, and feces. Lower airway specimen provides a more accurate yield. Recommend sending specimen for testing as soon as possible.
IgM to the Novel Coronavirus becomes positive 3-5 days after onset of symptoms. During the recovery period, IgG to the Novel Coronavirus increase by 4 folds or higher than in the acute phase.
Early stages usually present with small infiltrates and interstitial changes, more apparent in the peripheral of the lungs. Later on, radiographic evidence can progress to bilateral ground glass appearance, and diffuse infiltrates. Severe patients can develop significant consolidation in the lungs. (A supplemental guideline from frontline hospitals indicated that some critical patients develop “white lungs”). Pleural effusion is unusual.
- Suspected cases
Clinical suspicion can be made by the combination of contact history with clinical presentation.
- close contact with known infected individual within the past 14 days, traveled from or live in endemic areas within past 14 days, and patient is a member of a cluster appearance of infected individuals (2 or more cases within a small group such as family, office, classroom) within 14 days.
- Clinical presentation of fever and/or respiratory symptoms; or radiographic evidence that is consistent with 3(c); or in early stages of the disease with lower peripheral leukocytes and lymphocytes.
If a patient meets 1 criteria in i), and 2 criteria in ii); or all three criteria in ii), the patient is a highly suspected case.
If a suspected case meets one of the criteria of 1) RT-PCR positive for 2019-nCoV, or 2) genetic sequence highly consistent with 2019-nCoV, 3) Positive IgM or IgG to the Novel Coronavirus (2019-nCoV).
- Mild:
Mild clinical disease, no evidence of pneumonia on radiography.
Fever, respiratory symptoms, and pneumonia on radiography.
Any one of the three below in an adult:
- Tachypnea, RR>30
- SatO2 <=93% on RA
- PaO2/FiO2 <=300mHg (adjust for altitude)
- Chest radiography (XR or CT) showed >50% progression within 24-48 hours.
Any one of the 5 in children:
- Shortness of breath (<2mo, RR>=60/min; 2-12mo, RR>=50/min; 1-5yo, RR>=40/min; >5yo, RR>=30/min), without the effect of fever or agitation
- Breathing with accessory muscles, cyanosis, episodic apnea
- Excessive drowsiness, convulsion
- Refuse or difficulty feeding, dehydration
Any of the three below:
- Respiratory failure, requiring mechanical ventilation
- Syncope
- Other end organ damage requiring ICU care.
- Warning Signs of a Patient may Progress into Severe or Critical Types:
- Adults:
- Progressive decrease in peripheral lymphocytes
- Progressive increase in IL-6, CRP
- Progressive increase in LDH
- Children:
- Increase in RR
- Malaise, sleepiness
- Progressive increase in LDH
- Rapid progression in radiographic findings of bilateral or multilobar infiltrates, pleural effusion, or progressive worsening of symptoms in a short period of time
- <=3mo of age, chronic baseline diseases, primary or secondary immune deficiency
Need to rule other respiratory or systemic diseases that could mimic COVID19 (I am omitting that part. We all know)
(…. Other things about reporting, I am skipping here because it’s only relevant to the Chinese CDC)
8. Treatment
- Treatment locations: Suspected and confirmed cases should be treated in special hospitals which can carry out effective isolation and protection. Suspected cases should be in single isolation. Confirmed cases can be treated in shared rooms (with other confirmed cases). Critical cases should be treated in ICU.
- Treatment for Mild to Moderate diseases:
- Rest, supportive care, supply sufficient nutrition and fluid. Pay close attention to electrolyte balance. Close monitoring of vitals and SatO2.
- Monitor routine blood and urine labs, including CBC and diff, liver function, kidney function, CRP, CPK, coagulation, PaO2, and chest radiography. In indicated patients, can monitor inflammatory cytokines (such as IL-6).
- Ensure sufficient oxygen supply, with NC, face mask, or high flow O2 treatment. Can consider Hydrogen/Oxygen mixture (H/O2: 66.6%/33.3%).
- Some recommended anti-viral treatments to try (there is currently no proven anti-viral for this virus. The most promising one according to WHO officials is Remdisivir from Gilead):
- Alfa-interferon (5,000,000 U or similar dose, add 2ml sterile water) nebulized bid for adults, can be given in combination with any treatment below.
- Kaletra (Lopinavir/ritonavir) 200mg/50mg 2 tab bid for adults, for up to 10 days (monitor for GI side effect, such as nausea, vomiting, diarrhea, and elevated liver enzymes, QT prolongation)
- Ribavirin (recommended use in combination with Alpha-Interferon or Kaletra): 500mg IV bid-tid for adults, for up to 10 days
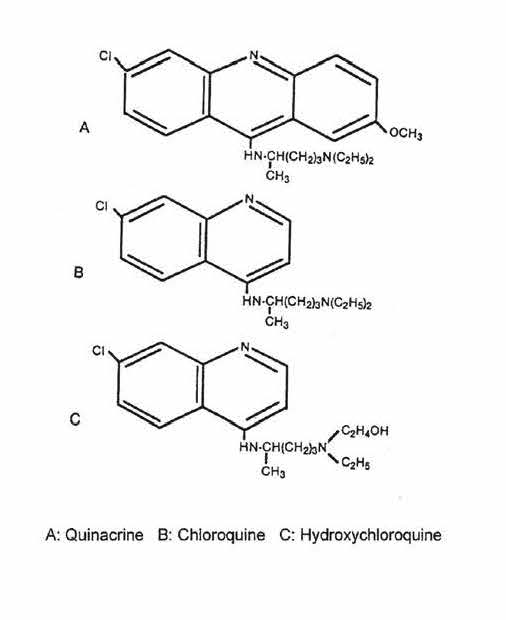
- Chloroquine Phosphate 500mg bid for adults >50kg; 500mg bid for Day 1 and 2, then 500mg qd for Day 3-7 for adults<=50kg; up to 10 days.
- (Gilead’s Remdisivir is currently under clinical study in China, so it’s not included in this guideline.)
- Close observation of side effect of each drug; do not recommend using >=3 antiviral treatments at one time.
- Take into consideration of gestational age of pregnant women. Choose medications with the least side effect during pregnancy.
- Avoid inappropriate usage of antibiotics, especially broad-spectrum antibiotics.
- Treatment for Severe and Critical Diseases
Principle of approach: On top of anti-viral treatment, actively prevent and treat complications, baseline chronic diseases, prevent secondary infection, and support vital organ function.
- Continue with treatment of Mild to Moderate diseases as above.
- Respiratory support:
- O2 through NC
- O2 through face mask or high flow O2, non-invasive positive pressure ventilation if the patient is de-sating. If high flow O2, non-invasive positive pressure ventilation is not sufficient to alleviating symptoms or low SatO2 after 1-2 hours, or patient is deteriorating, start intubation and mechanical ventilation.
- Invasive Ventilation:
- Use pulmonary protective protocol (this part is too technical, so I am translating the paragraph verbatim): use low volume ventilation approach (6-8ml/kg ideal body weight); and low pressure (airway plateau pressure <=30cm H2O), to decrease ventilator related pulmonary trauma. While maintaining airway plateau pressure<=35cm H2O, consider using high PEEP. Maintain warmth and moisture of airway. Try to avoid prolonged sedation, wake patient up and start pulmonary rehab as soon as appropriate. Majority of patients have asynchrony with mechanical ventilation, recommend sedation and muscle relaxant (paralytics?) when indicated. If patient has high amount of airway secretion, choose frequent airway suctioning under air-tight condition. Use bronchoscopy to remove lower airway secretion as indicated. (This recommendation is probably due to recent autopsy results showing significant airway obstruction with unusually thick and viscus mucus and mucus plugs)
- In severe ARDS patients, recommend pulmonary re-ventilation, when allowed, should have 12hr/day prone position ventilation. If still deteriorates, consider ECMO as soon as indicated: 1) When FiO2>90%, Oxygen Index is lower than 80mmHg, continuous for 3-4 hours, 2) Airway plateau pressure>=35mmH2O. Isolated ARDS patients should use WV-ECMO. ARDS patient needing cardiocirculatory support, use VA-ECMO. When cardiopulmonary function improves and baseline diseases are controlled, consider withdrawal of ECMO.
- Circulatory support: Improve microcirculation, use anticoagulants as indicated. Watch closely the patient’s heart rate, blood pressure, and urinary output. Watch Arterial Blood Gas closely, and arterial pH. Monitor with Echocardiogram, Doppler, PiCO. Keep patient at volume neutral. If the patient shows signs of increase HR>20% of baseline, or BP decrease by 20% baseline, or decrease urinary output, and peripheral circulatory insufficiency, consider workup for sepsis, GI bleeding or CHF.
- For patients with acute renal insufficiency, rule out low blood volume or medication side effect. Patients with severe renal insufficiency should go on continuous renal replacement therapy.
- Recovering patient’s plasma transfusion, consider in rapidly progressing patients, or patient in severe and critical stages (I don’t think it pertains to the US patient population now since the epidemic in US is just starting. Even in China, it’s a very limited resource).
- Plasmapheresis: consider in treatment in early to mid-stage Cytokine Storm patients, and patients in severe to critical stages of the disease.
- Immunotherapy: for patients with bilateral diffuse pulmonary infiltrates, or patients in severe to critical stages, if blood IL-6 level is elevated, can try Tocilizumab. Initial dosage of Tocilizumab is at 4-8mg/kg. Recommended initial dosage is at 400mg, diluted by 0.9%NS to 100ml, infused over >1hr. Patients without significant improvement after the initial dose, can have a second dose after 12 hours. Total dosage should not exceed twice total, and single dosage should not exceed 800mg. Watch for allergic reaction. Patients with TB or other active infection should not use Tocilizumab.
- Other treatment: for rapidly deteriorating pulmonary or cytokine storm patients, consider glucocorticoids 1-2mg/kg. Be judicious in using glucocorticoids as it can suppress the body’s immune system and slow the clearance of the virus. Use probiotics to prevent secondary infection through GI tract. Children with severe or critical disease can consider IVIG. Pregnant patients with severe or critical disease should consider active delivery, through C-Section when appropriate.
- Patients usually have significant anxiety. Pay attention to patient’s psychological health. Sedation may be indicated.
(…. Then a section regarding Chinese herbal medicine, which doesn’t pertain to us. I skipped)
9. Discharge Criteria and Post-Discharge Care
The patient can be discharged if they satisfy all below:
- Normal body temperature for >3 days.
- Significant improvement in respiratory symptoms.
- Radiographic improvement.
- Consecutive 2 negative RT-PCR for 2019-noCoV test on nasopharyngeal or sputum samples, at least 24 hours apart.
Discharge care:
- Monitor patient for another 14 days (basically stay at home after discharge, wear a mask at home if living with others, avoid close contact with family members, and avoid going to public areas for another 14 days after discharge).
- Return visit in 2-4 weeks.
10. Pathological Changes (This entire section is new)
The pathological findings are based on limited biopsy and autopsy reports:
- Lung
Different degrees of consolidation. Alveoli are filled with serous exudate, fibrinous exudate, and hyaline membrane formation. Monocyte, macrophage infiltrate, and Langhans cells are seen. Significant hyperplasia of type II alveolar epithelial cells. Some desquamation is present. Inclusion bodies can be seen within macrophages and type II alveolar epithelial cells.
Alveolar congestion and edema can be seen. Infiltration of monocytes, lymphocytes and formation of hyaline thrombus in blood vessels are seen. Pulmonary hemorrhage and necrosis, and hemorrhagic infarct are seen. Some alveoli exudate and interstitial fibrosis can be seen.
Some desquamation of bronchial mucosal epithelium. Mucus plugs are seen in bronchioles. Some alveoli suffer from over-inflation, fracture of septal walls, and cyst formation.
Coronavirus particles can be seen in bronchial epithelial cells and type II alveolar epithelial cells under electromicroscope. RT-PCR positive for 2019-nCoV.
- Spleen, Hilar Lymph nodes and Bone Marrow
Spleen is significantly smaller. Lymphocyte count is significantly reduced. Focal hemorrhage and necrosis is present. Macrophage hyperplasia and phagocytosis is present in spleen. Reduction of lymphocyte and necrosis are seen in hilar lymph nodes. CD4+ and CD8+ are both reduced in spleen and lymph nodes. In the bone marrow, hematopoietic cells of all three lineage are reduced.
Cardiomyocytes showed degeneration and necrosis. Small amount of interstitial infiltrate of monocytes, lymphocytes, and neutrophils can be seen. Desquamation, endothelial inflammation, and thrombosis are seen in some vessels.
The liver is enlarged, and dark red in color. Hepatocyte degeneration and focal necrosis are seen with neutrophilic infiltrate. hepatic sinusoidal congestion, infiltrate with lymphocyte and monocyte and microthrombi are seen in hepatic portal system. The gallbladder appears highly filled.
Proteinaceous exudate is seen in glomeruli. Degeneration and desquamation of renal tubular epithelium. Hyaline casts can be seen. Interstitial congestion, microthrombi, and focal fibrosis can be seen.
Cerebral edema, hyperemia, and neuron degeneration are seen. Focal necrosis of adrenal glands is seen. Esophageal, gastric, and intestinal mucosal epithelial degeneration, necrosis and desquamation is seen in various degrees.