Andrew Ripps and his Bendcare company have risen from COVID and will conduct another “Summit” in Colorado Springs, at the luxurious Broadmoor, next week. I was so moved by the summit I attended in January, I set about to compose a response, which I’ve sat on till now. I’m getting it out now, as the new summit will almost certainly leave me with new impressions. I’m particularly interested in what the ever foreword-thinking Dr. Ripps will have to say about rheumatology practice in the world of coronavirus, especially how you can still make money, a mission at which my own Division has miserably failed.
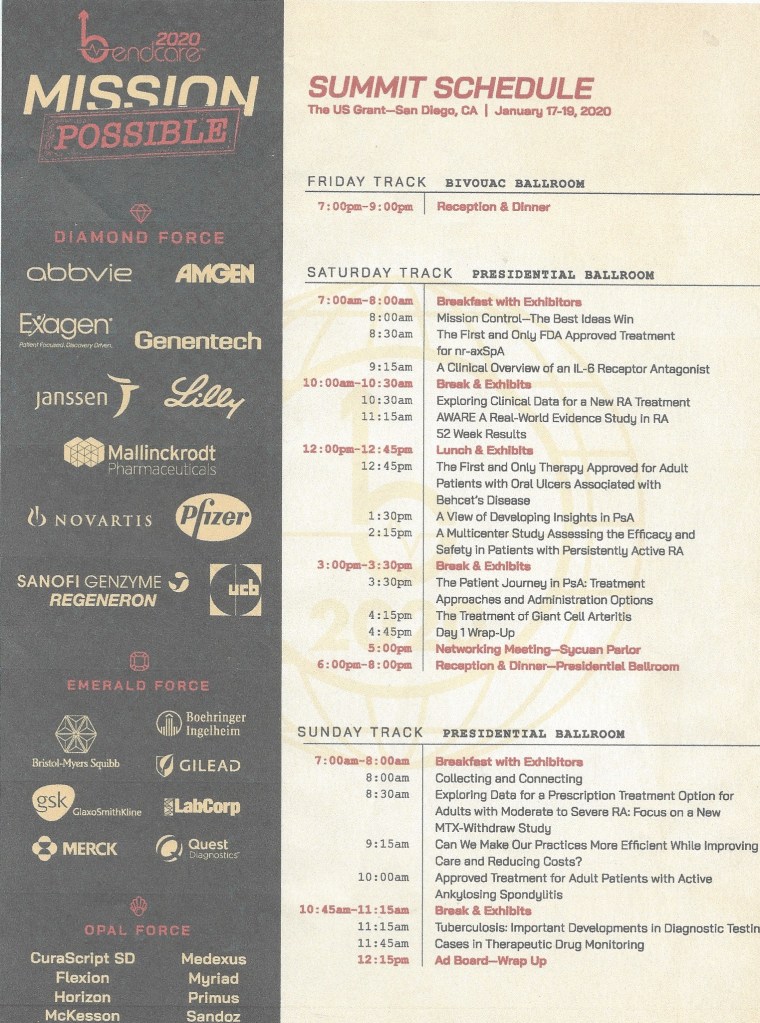
Thoughts on the Bendcare Summit, US Grant Hotel, San Diego 1/17-19/20
The invite came out of the blue. On a cold day in early November somebody named Michael Prondecki wants to fly me to San Diego in January and put me up at a luxury hotel to participate in the first of the year “Bendcare Summit” with 80 of my peer “top Rheumatologists” from around the country. Few other details, but there’s CME involved and he’s not asking me to talk. To San Diego in January could easily be added “my San Diego”, e.g. LaJolla, with a chance to revisit some of the fun of those 3 months Kathy and I spent there 3 winters ago on my UCSD sabbatical. I quickly emailed Ken Kalunian, my friend and UCSD host, to ask if these guys were legit. When his affirmative answer came, I could no longer sit through the ever more boring seminar at the Ford school to rush home to my computer and accept my invitation while making further flight and AirBnB plans. I’d texted Kathy during the seminar and she was all in. Turns out Prondecki had been peppering me for months with invites to other great locations. I think it was the San Diego that got my attention.
Set we were soon for a DTW-SAN Friday 1/17, two nights at US Grant’s son’s hotel, then 3 nights at an AirBnB near LaJolla’s rocky and wondrous Windnsea beach. It turned out to be even more of a trip than that, which I’ve written about earlier in this blog. (https://theviewfromharbal.com/2020/01/17/way-too-early-on-a-friday-morning-january-17th-a-pre-travelogue/, https://theviewfromharbal.com/2020/01/21/brady-in-pb/, https://theviewfromharbal.com/2020/01/22/another-hard-day-in-lj/)
Although it seemed to take forever on the twisty-turny limo ride from SAN to the US Grant, we got there, got checked in, were challenged by the ice machine situation (see https://theviewfromharbal.com/2020/01/29/ice-at-the-us-grant/), but got spruced up enough to go to the welcoming walking dinner/reception. I didn’t recognize a single face. Most of us were older. Kathy and I struck up conversations with a few, particularly an outdoorsy guy with a pony-tail from Minneapolis (all of us escaping the cold), as we wandered from table to table stuffing and drowning ourselves. My fear of being found out as clinically inactive (I wasn’t retired yet) never materialized, and by the looks of some wandering about, it was clear many were ever looking forward to the 8th of each month.
Morning brought entry into the big meeting room, with mounds of sumptuous breakfast fare surrounding the meeting tables, the whole roomed rimmed by colorful displays of the supporting pharmaceutical companies, each manned during breaks by the attractive personable female (and some male) representatives of each respective company.
There was to be no scrambling for seats, as all participants were assigned a place.
There I was, seated next to the Klash. He was one of my dear friend and all-time scopy buddy Ken Kalunian’s first fellows who had joined me on several mastheads. We’d known each other a long time and kept in touch. Currently in private practice in Torrence, he was intently into this stuff as he desired to transform his practice but was being held back by some more conservative partners. Spread before us were several tchotchkes, including a program folder with an actual phonograph record inside, a book we should all read (but I haven’t yet: Daniel Coyle’s The Culture Code), a pen that is also a USB drive, pretty cool, a penlight that shone the Bendcare logo like Batman’s searchlight, and in that mysterious red and black leather container, a reusable metal straw complete with cleaning brush. Taking care of the earth is so cool nowadays. The retro angle pervaded, from the references to the old “Mission Impossible” (not the Tom Cruise remakes), to the rotary phones and old desks in the projections and old-looking phonograph record players on each desk. For us at this Summit, it was “Mission Possible”, transforming our practices with Bendcare’s assistance. We were all in this together.

Some assembled agents take their briefing:

The program began with a wild animated feature that sought to portray each of us a superhero fighting against those forces that made clinical rheumatology less fun, less lucrative, and less satisfying to our patients nowadays. Who wouldn’t buy in to a program that would do that? Dr. Ripps himself, who made his original fortune organizing the first boutique practices, a pharmacist by training, stepped up with some rousing general comments. His aim was to achieve “healthier healthcare”. Finishing by saying we should all “kill, crush, and destroy” those forces impeding us, he had us in a lather that would last all weekend.
The program which followed could have come from any general rheumatology CME course. All speakers were seasoned and adept veterans of such presentations. Each speaker dealt faithfully from their deck of stylish, detailed, industry-provided slides. Some speakers went off-script to varying degrees with one, Dr. Wells, displaying the zeal of an old time gospel preacher for a most entertaining show.
Punctuating interest in the program, at least among the male participants, was the gorgeous young woman who introduced each speaker: pretty, pouty and petite, her straight long black hair flowed all the way down the back of her snug red dress as her luminous eyes flashed across the darkened room, seeking out the uninvolved. She also had the duty of passing around the microphone in the Q&A after each talk. She used the empty chair next to me to rest the large padded cube of a microphone she would toss about to participants who had questions for the speaker. At times, she would rest herself in that chair, holding the microphone in her lap as I silently sighed my wish I could be that microphone. I’m sure the prospect of sidling up to her encouraged audience participation. Ripps sure knows what he’s doing.
Not just at breakfast, but at lunch and dinner too, in front of the displays, tables bearing silver vessels laden with food more beautiful and delicious than the drug reps it displaced would appear. I approached lunch with the ravenous appetite of someone who had been digging ditches all morning rather than sitting and listening to talks.
By mid-afternoon, Klash had cracked the code. He’d actually sat down with one of the Bendcare folks to see what their deal was all about. He produced for me this mandela.
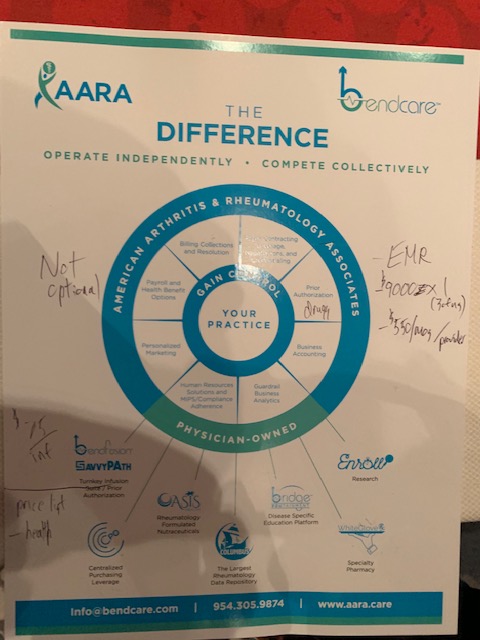
Bendcare offers all sorts of bundled services. You actually buy in by joining American Arthritis and Rheumatology Associates (AARA, don’t try to find ’em on the net), a parent corporation. Costs $3000 up front, then $550/mo. Bendcare makes most of its money on your data, which I’m too much of a boomer to understand. But they have the biggest base of patient outcomes data of anyone in the world. Must be important to somebody.
As the afternoon wore on, more and more of the participants opted for 65o and sunny San Diego over our dark ballroom and presentations from slide decks. The crowd was so sparse by mid-afternoon that we all got a text message before the 3 o’clock break pleading us to return for the day’s remaining speakers. My break was highlighted by a lively conversation with a pretty blonde, 6’ plus 4” heels, drug rep (I forget the product), followed by a reminder I was really loved when I caught my wife working away at an outdoor table at the fish house across the way, kitty corner from the hotel, having taken the time to order a beer for me before I arrived. I still tore myself away to finish the afternoon. Not all the participants fared so well in the late afternoon sessions.

In the “happy hour” that supervened between session and dinner, Ripps started to get down to the nitty gritty of what it meant to sign up with Bendcare. The room was well populated with converts, if not too well stocked with booze, who stood up and testified how their practices had changed for the better. Questions from the curious were entertained, and a lot of us trickled out to sit at the hotel bar where we actually had to pay for our drinks but could at least talk to each other.

Dinner was a lively affair, with fired up participants flying all over the place with full plates and drinks, gabbing away. My friend and colleague Elena was there and we plotted how we could break free of the U, start our own practice, and make millions with Ripps’ help. Ripps was circulating and I sought him out to shake his hand and thank him. I offered that he was helping to alleviate the rheumatologist shortage by enticing the disgruntled retired to reenter the workforce with the prospect of facing a more friendly environment under his wing. He liked that.

Sunday was a half day to be endured until Mike Prondecki handed you your check. Ripps’ IT guy took the stage and tried to explain how big data is so important. Still not getting it. But Bendcare offers an EMR far more friendly than EPIC. I’m all for that.
Kathy and I were itching to get up to La Jolla so we could attend services at La Jolla Presbyterian (https://ljpres.org/), the incomparable Pastor Cunningham presiding. Yes, we were looking forward to the better part of a week on Windnsea Beach, but we really did want to go to church. So no AS update or TB for me. Mike was kind enough to slip Kathy my check anyway. There’ll be more of these Summits. They allow you two a year, and they’re all in fabulous locations https://www.bendcare.com/summits/, returning participants encouraged. You rheumatology docs out there with any sort of interest should sign up. They’re not selling Florida timeshares. Just hope, and we all could use a dose of that.
So Bendcare is o.k. by me. If I do get back to work by starting a new private practice, I’ll be leaning on them heavily. Long as they love me, it’s alright. https://www.youtube.com/watch?v=gO35iRn67i4















