On March 4th, in a 9 page (once translated) document, the Chinese Health and Public Health Ministry put out their 6th revision of its Guideline on Novel Coronavirus Disease (COVID-19) Diagnosis and Treatment. I put the full guidelines on my blog Thursday.
Only 2 small sections mentioned anything about drug treatment. But they have found some things that seem to work, at least for some cases.
First, lets look again at the treatment recommendations, then I’ll explain each drug to the best of my ability.
- Some recommended anti-viral treatments to try (there is currently no proven anti-viral for this virus. The most promising one according to WHO officials is Remdesivir from Gilead):
- Alfa-interferon (5,000,000 U or similar dose, add 2ml sterile water) nebulized twice daily for adults, can be given in combination with any treatment below.
- Kaletra (lopinavir/ritonavir) 200mg/50mg 2 tablets twice daily for adults, for up to 10 days (monitor for GI side effect, such as nausea, vomiting, diarrhea, and elevated liver enzymes, QT prolongation – an electrocardiogram feature)
- Ribavirin (recommended use in combination with Alpha-Interferon or Kaletra): 500mg IV twice daily-three times daily for adults, for up to 10 days
- Chloroquine Phosphate 500mg twice daily for adults >50kg; 500mg twice daily for Day 1 and 2, then 500mg qd for Day 3-7 for adults<=50kg; up to 10 days
- (Gilead’s remdesivir is currently under clinical study in China, so it’s not included in this guideline.)
- Close observation of side effect of each drug; do not recommend using >=3 antiviral treatments at one time.
Remsdesivir was developed by Gilead to treat Ebola, a filovirus that like COVID-19 has an RNA genome, but is smaller, both physically (80%) and by length of genome (2/3ds), plus its RNA is a negative strand so it must be duplicated before taking over the host cell. And Ebola is not as hardy as the coronaviruses, as it must ride in the host’s bodily fluids to be transmitted. Remsdesivir works by acting as a nucleotide analog of adenosine (remember the 4 letters of the language of God: ATGC https://www.amazon.com/Language-God-Scientist-Presents-Evidence/dp/1416542744/ref=sr_1_1?crid=149QA07AXVVM1&keywords=the+language+of+god&qid=1584884234&sprefix=the+langua%2Caps%2C179&sr=8-1), taken up into the new RNA being made by the virus which can not then be translated and direct the manufacture of new virus proteins, a slick little chemical vascectomy for Mr. Corona. In the lab, it’s been shown to suppress the replication of a number of RNA viruses, including the coronaviruses responsible for SARS and MERS. In late January 2020, remdesivir was administered to the first US patient to be confirmed to be infected by SARS-CoV-2, in Snohomish County, Washington, for “compassionate use” after he progressed to pneumonia. While no broad conclusions were made based on the single treatment, the patient’s condition improved dramatically the next day, and he was eventually discharged https://www.nejm.org/doi/10.1056/NEJMoa2001191. Clinical trials of the drug in active COVID-19 infection are underway in China and as a 50 site multicenter study coordinated out of the University of Nebraska https://www.nih.gov/news-events/news-releases/nih-clinical-trial-remdesivir-treat-covid-19-begins, https://clinicaltrials.gov/ct2/show/NCT04280705. In this trial, patients in the treatment arm will receive 200mg remsdesivir IV on day one then 100 mg IV daily to complete a 10 day course. Other trials are set to commence in Asia, and may be ongoing already. Some will test a 5 days course. Gilead and the investigators expect usable outcomes data in April. Market analysists who study such things expect Gilead to price remsdesivir at $900-$1000 per course https://www.biopharmadive.com/news/coronavirus-remdesivir-gilead-antiviral-drug-covid-19/573261/.
Alfa-interferon is a much older therapeutic agent. Not really a “drug”, it is coaxed out of cultured E.coli and purified to look just like the human alfa-interferon produced in response to viral infections. There are three different interferon protein classes, alpha, beta and gamma. Alpha interferons are produced by fibroblasts and monocytes exposed to viruses and viral components, boosting the activity of immune cells around them. Beta and gamma classes come out in response to other of the host’s immune signalling proteins (cytokines). One of the reasons you don’t get sick again right after recovering from a viral infection is that your circulating interferon levels are sky high. Over 40 years ago rheumatologists in Finland administered interferon to 6 patients with rheumatoid arthritis, seeing encouraging results. They were trying to mimic the effect seen after a measles infection where patients often transiently improved. Larger controlled trials could not confirm the positive effects seen, and the agent never entered the anti-rheumatic armamentarium, except for some promising observations with Behçet’s disease. However, its anti-proliferative and anti-viral properties have been directed at: hairy cell leukemia, malignant melanoma, AIDS-related Kaposi’s sarcoma, follicular non-Hodgkin’s lymphoma, and condyloma acuminate (all FDA approved) and also chronic myelogenous leukemia (CML), renal cell carcinoma, neuroendocrine tumors (carcinoid syndrome; islet cell tumor), multiple myeloma, non-follicular non-Hodgkin’s lymphoma, cutaneous T-cell lymphoma, desmoid tumor, polycythemia vera, essential thrombocytopenia, and idiopathic thrombocytopenia purpura. It was the first agent to have any success against hepatitis C, and when ribavirin came along, combination therapy of ribavirin with interferon alpha was standard of care. During courses of treatment, some patients with presexisting autoimmune diseases saw them flare, and new autoimmune diseases emerged in others. Flu-like symptoms are common after injection. The agent can now be given in nebulized form, although the vehicle used can sometimes cause cough, likely limiting its use in patients already having respiratory difficulties.
Kaletra (lopinavir/ritonavir) 200mg/50mg was developed for treatment of HIV, approved by the FDA in 2000. Both lopinavir and ritonavir inhibit HIV’s protease, an important molecule it makes the invaded cell synthesize early in infection. The 9 genes of HIV direct manufacture of 15 different proteins. The protease is responsible for modifying all the other HIV proteins being manufactured that will make up the virus’s coat, blast exit of new viruses from the cell, and mediate entry into new cells. The two drugs are given in combination because ritonavir increase the concentration of lopinavir in the body. Neither drug given alone can achieve effective levels with oral dosing. There are several other drugs of this class, including ritonavir (Norvir), nelfinavir (Viracept) and saquinavir (Invirase, Fortovase). Together, these drugs have revolutionized the treatment of HIV-1, converting it from a dreaded killer to a manageable chronic long term disease. Kaletra (and the rest of the protease inhibitors) are expensive, with AbbVie offering a savings program worth $400/month to eligible patients.
Ribavirin is an old drug, patented in 1971 and approved for medical use in 1986 to treat hepatitis C. It interferes with viral nucleic acid synthesis through molecular mimicry. Once phosphorylated in the cell, it mimics inosine 5′-monophosphate, which is critical in making one of those “language of God” letters: G (guanine), and inhibits the enzyme Inosine-5′-monophosphate dehydrogenase (IMPDH). RNA synthesis slows, and ribivarin monophosphate can be incorporated into new viral RNA leading to defective genes. Resistance can develop if the drug is given alone, so it is always given with interferon. While effective, it has largely been supplanted by newer medications (elbasvir/grazoprevir (Zepatier) glecaprevir/pibrentasvir (Mavyret), sofosbuvir/ledipasvir (Harvoni), sofosbuvir/velpatasvir (Epclusa).
I have just put on my white coat, complete with stethoscope in pocket, so I will be writing the rest of this piece with all the medical authority and experience I can muster.
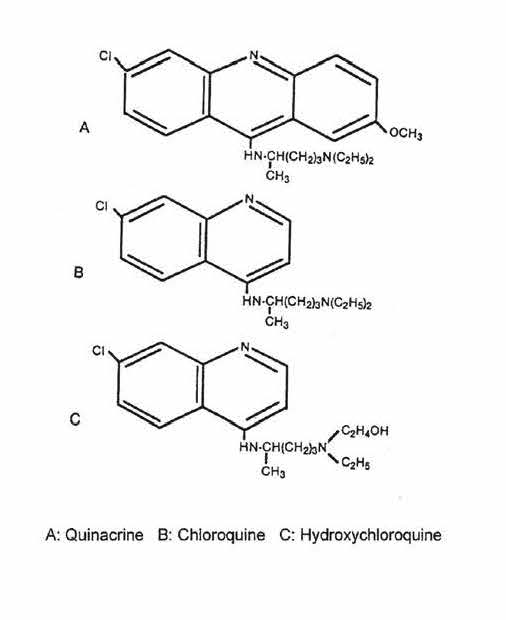
The remaining drug is this first discussion of drug treatments in the Chinese Guideline is chlororquine phosphate (Aralen). Although considered a product of an intensive U.S. research effort to develop an antimalarial alternative to quinacrine (Atabrine) during World War II, German producers of Atabrine had produced chloroquine phosphate in 1934 but shelved it as too toxic. GIs in the Pacific disliked that Atabrine turned their skin yellow, and especially didn’t like it when Tokyo Rose told them it would make them sterile (untrue). Noncompliance was a problem and many GIs died of malaria because they had not taken their Atabrine. Aralen was patented in 1941 and GIs were taking this non-yellowing but effective drug by 1943. The Journal of the American Chemical Society describing details of synthesis of Aralen was kept by the Defense Research Council from being published till after the war. The drug’s antirheumatic effects were noticed in patients with rheumatoid arthritis and lupus who happened to take the drug for malaria prophylaxis. Aralen was highly effective for malaria for a while, but resistant strains of Plasmodium began to emerge by the mid-late 50s. Hydroxychloroquine (Plaquenil) was approved for malaria in 1955, and was better tolerated but no more effective against malaria. Plaquenil became the preferred antirheumatic antimalarial, and many practicing rheumatologists now worry that the push for use of Plaquenil for coronavirus treatment will deprive their patients of an important drug. I have covered use of antimalarials for coronavirus already in my blog (“My Corona” 3/14/20, “Plaquenil for Corona” 3/19/20, and “How Plaquenil may work” 3/20/20).
But wait there’s more! Later in the guideline, under “Treatment for Severe and Critical Disease”, is this section:
Immunotherapy: for patients with bilateral diffuse pulmonary infiltrates, or patients in severe to critical stages, if blood IL-6 level is elevated, can try tocilizumab. Initial dosage of tocilizumab is at 4-8mg/kg. Recommended initial dosage is at 400mg, diluted by 0.9%NS to 100ml, infused over >1hr. Patients without significant improvement after the initial dose, can have a second dose after 12 hours. Total dosage should not exceed twice total, and single dosage should not exceed 800mg. Watch for allergic reaction. Patients with TB or other active infection should not use tocilizumab.
Tocilizumab (Actemra) is a humanized (made in animal cells then having the animal traces chopped off) monoclonal antibody to the interleukin-6 receptor. Interleukin-6 is one of the main cytokines pumped out of the liver in acute inflammation, produces a number of negative downstream effects when it binds to its receptor, an interaction prevented by Actemra. It is highly effective in rheumatoid arthritis, and was improved for use there in 2014. More recently, it has been shown be effective in giant cell arteritis (temporal arteritis) an inflammatory disease affecting larger arteries, primarily of the head and neck, in older people. It has found some use in “cytokine storm” an inflammatory emergency that can be seen in cancer patients that can occur when chemotherapy is so effective that there is extensive death of the cancer and a huge inflammatory response mounted against it. Something similar can occur in the lungs of patients infected with COVID-19. Actually, it is very old news that severe lung damage in virus infections is mediated more by the body’s immune response to the infection and dying lung tissue than to the infection itself. This was seen in the lungs of people dying of pneumonia during the influenza pandemic of 1918. With IL-6 being a prime mediator of this response, the reasoning goes that blocking this response might minimize and even reverse the damage. The dosing regimen described is different form that used for RA or GCA, where the agent is infused every four weeks.
The Guideline also mentions giving high doses of prednisone to patients in respiratory distress, which happens all the time in medicine anyway.
So those are the weapons the Chinese are employing in the fight against COVID-19. With the already wide distribution of this Guideline, no doubt some combinations of these treatments are being used in American hospitals now. The story that’s going to break first is the Plaquenil/Aralen thing. The FDA is front burner on at least one of them. The winner may be the one whose manufacturer can turn up the synthesis vats fastest.
I hope you readers take away some optimism that help is not only on the way, it’s actually already here. All of these drugs have some undesirable side effects long term, proving again it’s not nice to fool mother nature. But all these are for a very short term course. And let’s pray we can use that term to describe the remaining life of COVID-19